Spiritual Well-being and Quality of Life for Patients Undergoing Chemotherapy
Pancreatic Cancer Blog – Commentary on Articles and AbstractsHere is where we take complex medical articles and break them down into language you and I
For over 22 years pancreatica.org has provided current, credible, and comprehensive information to those in need.
Cancer Patient’s Alliance is a 501(c)(3) non-profit organization. All donations are tax-deductible.
94% of all revenue goes towards our programs, with only 6% towards MANAGEMENT AND GENERAL EXPENSES.
Surgery for adenocarcinoma of the pancreas is only offered to patients whose tumor is localized and meets other criteria. Only about 15-20% of those individuals with pancreatic cancer will be found to be eligible for surgery. In these cases, surgical resection (removal) of the tumor from the pancreas (and resection of the pancreas and select surrounding tissues) gives the best chance for a cure and generally confers a better overall prognosis in contrast to medical therapy for pancreatic cancer. This is one reason why so much effort is given in pre-operative testing for pancreatic cancer to try to identify those patients who may be good candidates for surgery. Another reason for such care is to avoid offering unnecessary surgery to patients who are already ill.
At surgery, the first job of the surgeon is to assess the nature and extent of the pancreatic cancer – to verify if the patient is a true candidate for surgical resection. If the pancreatic cancer has advanced further than the pre-operative testing has indicated (which is not uncommon), then certain palliative surgical measures as noted below (aimed at symptomatic relief) may be offered, but the resection would typically NOT proceed.
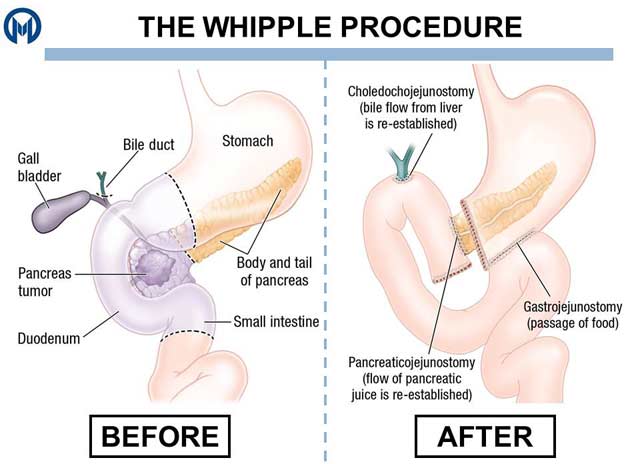
The resection, known as the Whipple operation / procedure (or pancreaticoduodenectomy) is typically done for patients who have tumors which are located in the head of the pancreas or which are located in regions adjacent to the head of the pancreas. There are a number of variations of the Whipple procedure. The classic procedure, a modification of the surgery described by A.O. Whipple and his colleagues in 1935, is a fairly extensive and somewhat complicated two-step process whereby certain key structures in the surrounding vicinity are removed (including that portion of the involved pancreas), followed by a kind of surgical bypass-reconstruction, in effect re-routing the digestive tube around the affected area.
One of the fundamental questions among researchers and surgeons relates to the necessary scope and extent of the pancreaticoduodenectomy surgery. Which tissues should be resected (and what are the optimal amounts to be taken) in order to get the best chance of survival, as balanced against quality-of-life issues. This topic is controversial and there has been a see-sawing back and forth over time between advocates of more radical procedures and those who advocate less extensive surgery.
If the pancreatic tumor is located in the tail of the pancreas, often that portion of the pancreas will be removed along with the nearby spleen.
The Whipple surgery itself can take several hours and is often grueling for the surgical team. The region of the body where the pancreas lies is very busy and complicated anatomically. Not only is the normal anatomy complex, but individual anomalies are frequent among the various blood vessels and ducts in the area. However, one of the great successes in the treatment of pancreatic cancer has been the improvement in mortality related to the Whipple surgery. The mortality was extremely high even a couple of decades back, but this has dramatically improved. Now, operative mortality related to the Whipple procedure is variously reported as 2-3%, but in some major U.S. institutions the more recent operative mortality has been reported at less than 1%.
Nevertheless, recovery can be an ordeal for the patient. Serious complications following surgery are still effect up to one-third of patients. These include the development of fistulas (false channels), and leakage from the site of the bowel reconnection. The judicious placement of surgical drains may tend to reduce the incidence of these kinds of complications. The survival of patients who received the Whipple procedure in one study (from a very experienced Johns Hopkins team) were reported out in 1995 as a 21% five-year survival rate, with a median survival of 15.5 months.
If it is determined that the pancreatic cancer is too advanced to make surgical resection a viable option, then certain palliative procedures or surgery may be offered. These are typically targeted at the primary symptoms or causes of symptoms in pancreatic cancer: pain, small bowel obstruction and jaundice due to physical compression of the bile duct. Thus a nerve block of the celiac nerve plexus may be done (for pain), and/or a gastrojejunostomy (stomach bypass) surgery, and/or bile duct bypass surgery. Stents (inner wall supports) may be placed for certain of these procedures.
There are two principles that need to be introduced at this time. Adjuvant therapy is a concept that connotes the practice of giving medical and/or radiotherapy after surgery for pancreatic cancer to help augment the effects of surgery. And neoadjuvant therapy is the term that describes the practice of giving such treatment prior to surgery for potentially resectable (surgical removal) pancreatic cancer disease. For long while it has been fairly common practice in the U.S. to give chemoradiation (chemotherapy plus radiation) as adjuvant treatment after the Whipple procedure surgery for pancreatic cancer. This practice is based on the results of a 1985 landmark study which demonstrated an almost double survival advantage for those who received such therapy. The radiation aspect of this practice has challenged in recent times as offering no statistical survival advantage in pancreatic cancer. But this issue remains a controversy as some experts doubt the challenge.
The use of neoadjuvant therapy is an intriguing area of research in pancreatic cancer. According to some studies, chemoradiation may push back the pancreatic cancer enough to allow some patients (a minority) with apparent unresectable cancer of the pancreas who otherwise might not be candidates – to be eligible for surgery, and thus may offer some survival advantage to select patients.
The following are descriptions of titles of abstracts of medical journal articles that may be interesting or useful to those who are interested in further information about this topic.These abstracts can be searched Here.
James Abbruzzese, MD Chief, Medical Oncology Duke University
Markus Büchler, MD Chairman, Surgery Heidelberg University, Germany
Ralph Hruban, MD Director, GI / Liver Pathology Johns Hopkins University
Eileen O’Reilly, MD Associate Director for Clinical Research – Memorial Sloan-Kettering Cancer Center
Margaret Tempero, MD Chief, Medical Oncology University of California at San Francisco
All DONATIONS are tax-deductible
Our Philosophy About Pancreatic Cancer
Pancreatic cancer is a serious disease. Taking an aggressive rational stance at the earliest possible time, supported by the best medical team, and treated in the most appropriate manner gives the best chance for survival.
We believe in strong patient-physician bonds, scientifically-based treatment, and that comfort can come from knowing that everything that reasonably can be done – is being done.
That the best approach is meeting cancer of the pancreas head-on and armed with the best available information.

Regular giving can be an opportunity to pay tribute in honour of a loved one. Your monthly gift will go directly to promoting awareness, increasing education, furthering pancreatic cancer research aimed at early diagnosis and, helping patients and families impacted by the effects of pancreatic cancer.
Simply select “Monthly” after choosing the amount you would like to give on the donation form.

Most of our fundraisers, supporters, and volunteers, have been in one way or another, personally effected by this disease. We want to acknowledge what hardships you may have gone through (or are currently facing) and sincerely thank you for visiting our site!
Join us in our effort to fight pancreatic cancer. Donations go directly to promoting awareness, increasing education, furthering pancreatic cancer research aimed at early diagnosis and, helping patients and families impacted by the effects of pancreatic cancer. All Donations are tax-deductible.

Making IMPACT for Pancreatic Cancer Together!

MONTHLY MEMORIAL GIFTS:
Support Pancreatic Cancer Research!
Regular giving can be an opportunity to pay tribute in honour of a loved one. Your monthly gift will go directly to promoting awareness, increasing education, furthering pancreatic cancer research aimed at early diagnosis and, helping patients and families impacted by the effects of pancreatic cancer.
Simply select “Monthly” after choosing the amount you would like to give.
Cancer Patients Alliance is a 501(c)(3) non-profit. Initiatives include, ToFightCancer.com and Pancreatica.org. All Donations are tax-deductible.
Pancreatic cancer is expected to become the 2nd leading cause of cancer-related death by the year 2020. There are many reasons why the outcome for pancreatic cancer patients is much bleaker than for most other cancer types. There are no reliable methods to detect the disease early, and there are very few effective treatment options.
| There remains a dire need for more research and an increase in focused funding for pancreatic cancer. Your Donation will go directly to promoting awareness, increasing education, and furthering pancreatic cancer research aimed at early diagnosis. |
This year an estimated 57,600 Americans will be diagnosed with pancreatic cancer. Approximately 47,050 Americans are expected to die from the disease. There are many reasons why the outcome for pancreatic cancer patients is bleaker than for most other cancer types. There are no reliable methods to detect the disease early, and there are very few effective treatment options. Which is why we are so focused on supporting research for early diagnosis.
Together with You our Mission is to promote awareness, increase education, and further pancreatic cancer research aimed at early diagnosis.


CREATE YOUR OWN FUNDRAISER FOR PANCREATIC CANCER !
Create your own fun, choose something you already love to support pancreatic cancer! Simply set up your participation page, include the details of your fundraiser on your page, and get the word out!
Shop to Support Pancreatic Cancer !
Amazon donates 0.5% of the price of your eligible AmazonSmile purchases to help fight pancreatic cancer!
AmazonSmile is the same Amazon you know. Same products, same prices, same service. Simply use our Link to start shopping!


Best of the Pancreatic Cancer Blog
Pancreatic Cancer Blog – Commentary on Articles and AbstractsHere is where we take complex medical articles and break them down into language you and I
Pancreatic Cancer Blog – Commentary on Articles and AbstractsHere is where we take complex medical articles and break them down into language you and I
Pancreatic Cancer Blog – Commentary on Articles and AbstractsHere is where we take complex medical articles and break them down into language you and I
This study is basically looking at whether aspirin can make a chemotherapy drug called gemcitabine work better for pancreatic cancer. You’ve probably heard of aspirin; it’s the stuff you take for a headache or fever.
© 2024 Pancreatica. All rights reserved | Privacy Policy
312 Fountain Avenue, Pacific Grove, California 93950 | Phone: (831) 658-0600 | Fax: (831) 658-0518 | participate@tofightcancer.com